PROLYNX has numerous early-stage programs aimed at developing long-acting therapeutics, as well as one preclinical program working towards an IND and one clinical stage program in several Phase II trials. The preclinical program involves a long-acting anti-obesity agent (a long-acting semaglutide (Ozempic)) with a half-life of ~1 month called PLX821, and the clinical program involves a long-acting prodrug of the DNA damaging agent SN-38 called PLX038.
PLX821
PLX821 - a long-acting once-monthly semaglutide.
Semaglutide was attached to hydrogel microspheres by a cleavable linker with an expected in vivo release half-life of about 1 month. After a single subcutaneous dose, the pharmacokinetic parameters of released semaglutide and bodyweight loss were determined in mice, and results were used to estimate the dosing and pharmacokinetics of the released semaglutide in humans. The in vivo half-life of released semaglutide was ~36 days, and a single dose in diet-induced obese mice resulted in a lean-sparing body weight loss of 20% over 1 month, statistically the same as semaglutide dosed twice daily. Simulations indicated the microsphere-semaglutide would permit once-monthly administration in humans; moreover, it could maintain the therapeutic minimum concentration (Cmax), a new feature that could reduce adverse side effects or allow higher dosing. The same approach should enable the conversion of other lipidated peptides from once-weekly to once-monthly administration.
PLX038
PLX038 (PEG~SN-38) – A long-acting DNA damaging agent designed for use in cancers with a defective DNA damage response (DDR) and inhibitors of the DDR.
PLX038 (PEG~SN-38) is a long-acting PEGylated prodrug of SN-38, the active metabolite of the approved anti-cancer agents irinotecan (Camptosar®, CPT-11) and Trodelvy® (sacituzumab govitecan). SN-38 is a potent inhibitor of topoisomerase 1 (topo1) that causes replication stress, inhibition of DNA synthesis and DNA damage leading to cell death in susceptible tumors. As a long-acting DNA damaging agent, PLX038 causes synthetic lethality in tumors with DNA damage repair defects and enhances the effects of drugs that inhibit the DNA damage response (DDR), such as PARP inhibitors.
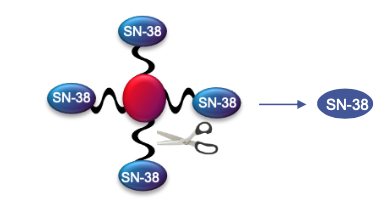
The long-acting PLX038 contains four SN-38s releasably connected to a 4-arm 40 kDa PEG through ProLynx linkers and slowly releases SN-38 in the physiological environment.
Topoisomerase 1 Inhibition. Inhibition of Topo1 leads to single-strand DNA breaks and leads to replication stress, inhibition of DNA synthesis, and ultimately cell death in susceptible tumors. It has been shown that continuous, protracted administration of topo1 inhibitors is advantageous over intensive bolus-delivery.
SN-38. SN-38 is one of the most potent inhibitors of topo1. SN-38 is too insoluble and has too short of a half-life to administer directly, and requires the use of soluble pro-drugs. Irinotecan, the paradigm SN-38 prodrug, is FDA approved and primarily used for treatment of colon cancer in combination with other agents. While highly effective, Irinotecan has many undesirable features:
- It is extensively metabolized so its pharmacokinetics and pharmacodynamics show high inter-patient variability.
- It is administered as a bolus infusion and shows a high Cmax – associated with toxicity – and short half-life.
- It requires activation to SN-38 in the liver, and as a consequence often shows severe GI toxicity due to extensive glucuronidation and excretion into the bile.
- The high toxicity and short half-life limit dosing regimens such that topo1 is not effectively inhibited for most of the dosing cycle.
Irinotecan is thus a sub-optimal prodrug of SN-38, with limited effectiveness as an antitumor therapeutic.
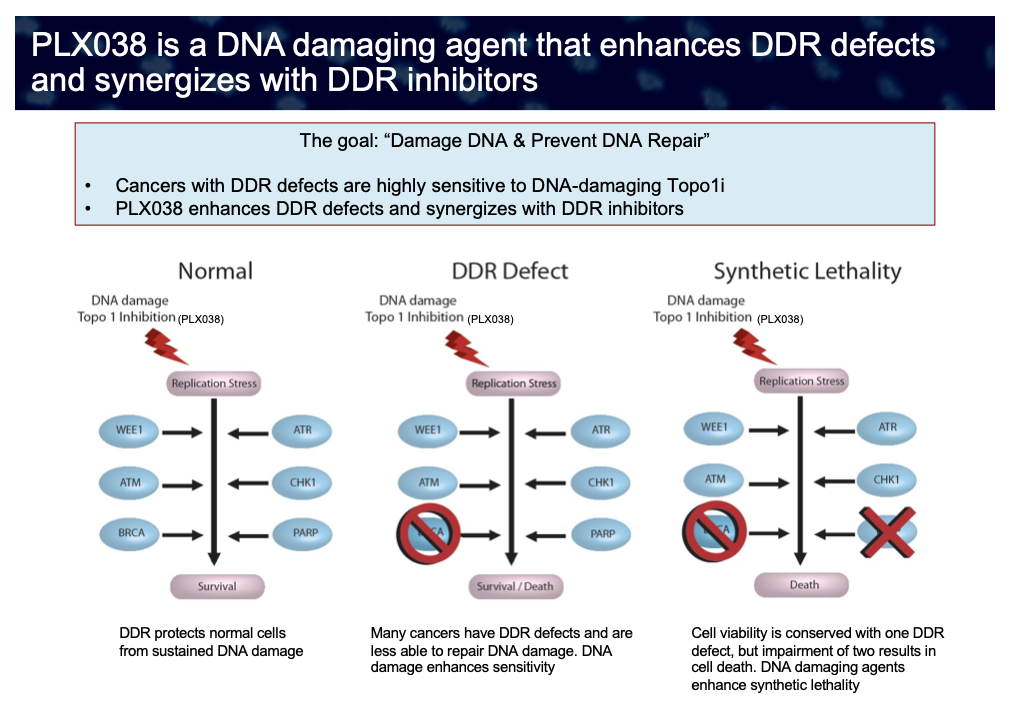
DNA Damage Response. Cells undergo thousands of DNA damage events each day. However, normal cells mount an effective “DNA damage response” (DDR) to recognize and correct the DNA damage with high fidelity, even in the face of DNA damaging agents such as topo1 inhibitors. However, many cancers have DDR defects and are less able to repair DNA damage, such as the situation with BRCA-deficiency. Also, even if tumor cell viability is conserved with one DDR defect, impairment of two or more – for example, in a tumor with a genetic BRCA deficiency treated with a PARP inhibitor – results in cell death by synthetic lethality. Cancers having a defective DDR display heightened sensitivity towards DNA-damaging agents – in particular PLX038 – due to a decreased ability to repair DNA damage resulting in lethality. Because of its superior pharmacokinetics, PLX038 has the potential to be used in combination with a variety of DDR inhibitors and in tumors which have pre-existing DDR defects. Tumors with a weakened DDR comprise a substantial portion of cancers and can be detected with use of appropriate biomarkers.
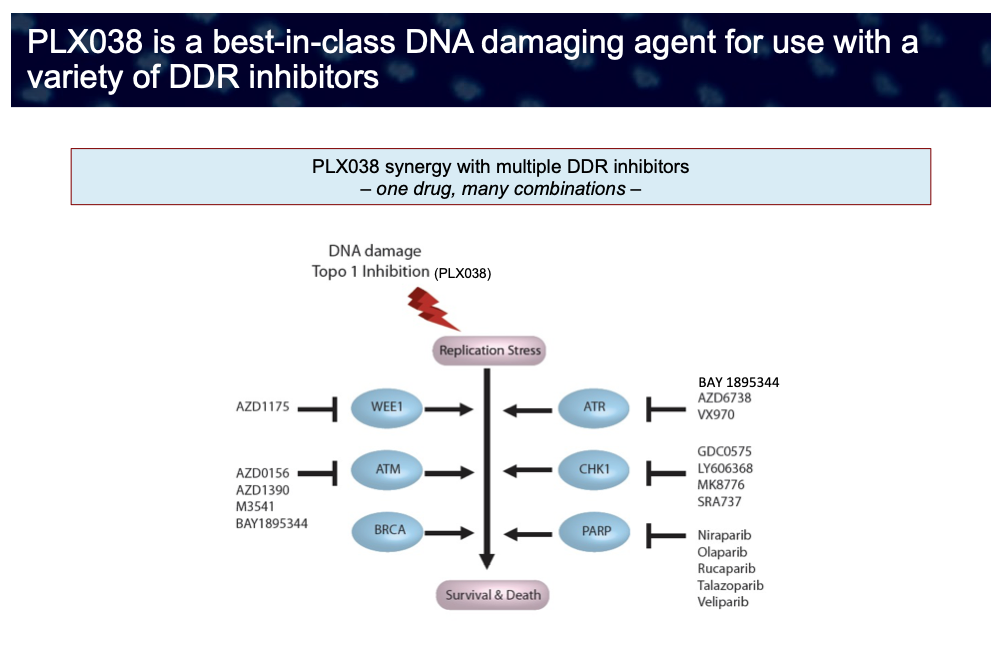
Defects in the DNA damage response have been recognized in many different cancer types. As a result, inhibitors of components of the DDR response which could cause synthetic lethality in such cells – such as PARP and ATR inhibitors – have assumed high importance in treatment of cancer. As such, numerous inhibitors of the DDR are in development, and it may be speculated that a single DNA damaging agent – such as PLX038 – might enhance the anti-tumor effects of many or all of them.
Thus, DNA damaging agents can be effective in (i) tumors with germline or somatic DDR defects – such as cells deficient in BRCA1/2, ATM or other DNA homologous recombination repair defects (i.e., cells with “BRCAness”), – and (ii) in cells where DDR deficiency is induced through chemical means, for example, in combination therapy with inhibitors of various DDR components, e.g., PARP, CHK1, ATM or ATR inhibitors.
PLX038 shows remarkable antitumor effects in preclinical models of human tumors with DDR defects and those treated with DDR inhibitors. For example, in the BRCA1-deficient human xenograft MX-1, a single, non-toxic dose of PEG~SN-38 completely inhibited tumor growth and resolved massive tumors.
PLX038 Differentiation and use with DDR inhibitors. PLX038 was designed to address the liabilities of Irinotecan and thus provide a superior anti-tumor agent. PLX038 exhibits a unique combination of the most desirable features of a topo1 inhibitor: (i) released SN- 38 has a very long half-life (5 days in human) and consequently a very low Cmax; (ii) SN- 38 is non-enzymatically released in the plasma rather than enzymatically in the liver, and so shows much lower glucuronidation and GI toxicity than Irinotecan; (iii) PLX038 accumulates in solid tumors, and (iv) shows high therapeutic efficacy.
PLX038 is a best-in-class DNA damaging agent for use with DDR inhibitors including, but not limited to, the approved PARP inhibitors, ATR inhibitors and inhibitors of other components of the DDR (e.g., CHK1, Wee1 kinase) now in development. Because of its long duration of DNA damage (~2 out of a 3 week cycle) compared to CPT-11 (~12 hr of a 3 week cycle), it provides a long time-window within which the DDR inhibitor may be optimally scheduled to achieve synthetic lethality.
Clinical trials of PLX038. PLX038 has been evaluated in a complete Phase I clinical trial at M.D. Anderson Center. It is currently being studied in several Phase I/II trials. These include patients with platinum resistant ovarian cancer at Mayo Clinic, CNS tumors at the NCI, and, in combination with the ATR inhibitor M1774, patients with ATM-deficient triple negative breast cancer at the Curie Institute. One objective of these trials is to identify biomarkers that will be useful in selection of patients mostly likely to respond to PLX038 therapy.